John Heron,formerly Assistant Director, British Postgraduate Medical Federation, University of London
Published in D.Peters (ed), Understanding the Placebo Effect in Complementary Medicine, London, Churchill Livingstone, 2001, pp 189-212.Outline
Inquiry paradigms
Cartesian anomaly
The downfall of positivism
A participatory worldview
Critical subjectivity and four ways of knowing
Methodology: co-operative inquiry
The body as a subjective-objective realityThe experiential bodyFormative intentionality of the experiential bodyFormative intentionality of illness and of recreating wellnessSymbolizing the experiential bodyThe formative power of others’ experiential knowingSupportive data
The relevance and limits of conventional medical research
The relevance of co-operative inquiry
A co-operative inquiry projectObstaclesMembership and rolesFirst reflection meetingCycles of inquiryCompleting the inquiry
Inquiry paradigms
Any method of inquiry presupposes an inquiry paradigm, which is a set of basic beliefs about the nature of reality and how it may be known (Guba and Lincoln, 1994; Heron and Reason, 1997). These are philosophical presuppositions of the method and are not derived from the method. However, the continued use of the method will start to show up the limitations of the paradigm underlying it.
The beliefs within an inquiry paradigm are revealed by three fundamental and interrelated questions. There is the ontological question, ‘What is the form and nature of reality’; the epistemological question, ‘What is the relationship between the knower and reality, and the extent of our knowledge of reality?’; and the methodological question, ‘How can the inquirer find out about whatever he or she believes can be known?’.
I will look at the participatory worldview in the light of these questions, then consider the implications of it for our understanding of the body, illness and disease, and for the future of medical practice and research, with a concluding focus on a project for using the participatory research method of co-operative inquiry. But first I consider the paradigm presupposed by conventional medical inquiry, and the limitations of it which are shown up by continued use of such inquiry.
Cartesian anomaly
The inquiry paradigm underlying conventional medicine and mainstream medical research is Cartesian and is fraught with the basic anomaly of the Cartesian view. For Descartes, mind and matter are independent substances: mind is nonspatial with none of the properties of matter, and matter is spatial with none of the properties of mind. The human physical body is included within the self-contained mechanism of the spatially extended material world. This is the objective world: a real world independent of our minds, operating according to causal laws, which we can find out by observing how its component parts work together. Such is the objectivist, positivist worldview of modern times, which Skolimowski (1994) calls Mechanos, the legacy not only of Descartes, but also of Bacon, Galileo, and Newton.
The anomaly in Descartes’ thinking is that, on the one hand, mind is nonspatial with no bodily properties at all, yet on the other hand he says that the mind is ‘very closely united’ with the body and ‘as it were intermingled with it’ (1641). Indeed, he makes the anomaly very specific: he says that the mind interacts with the body through the pineal gland. So, without apparently realizing the difficulty, he gives the nonspatial mind a precise spatial location in the body.
Medicine, typically in its use of drugs, perpetuates its own version of this sort of anomaly. With its therapy hat on, it wants to prescribe chemical substances which will have an independent effect within the assumed autonomous mechanism of the body. With its research hat on, it also has to acknowledge and allow for, by means of experimental design, the dynamic influence of mental belief on this mechanism via the placebo effect. Thus it wants to maintain, as the foundation of clinical practice, a view of the body as a self-contained physical system, so that it can deliver purely physical remedies for what it assumes to be purely physical defects. And it can only do this by also accepting as a guiding rule of effective and reliable medical research – in controlling for the placebo effect – that the body is not a self-contained physical system but one that can react strongly to mental events.
This is indeed a weird anomaly: the proven effect of mental belief on bodily functioning – the placebo effect – is acknowledged only so that it can be discounted in research and ignored in clinical practice. A remarkable and undisputed healing effect of unknown potential is dealt with in pejorative terms and is cast aside as an irrelevant distraction from the pursuit of competent medicine. Harvard Medical School anthropologist Arthur Kleinman asks: ‘Why is the placebo regarded as pejorative? Is it threatening to medicine?’ (de Cuevas, 1995). Clearly it is: it is threatening to the positivist, objectivist, mechanistic paradigm underlying medical research and practice; and hence to the powerful, unilateral, external control which medicine claims over people’s bodies. And the paradigm is cracking up under the strain of the threat.
A human body is not just an objective reality, part of the autonomous furniture of the universe. It is a subjective-objective reality. It is experienced from within and observed from without. When it is dysfunctional, there is both interior experiential illness and exterior observable disease process. Cartesian medicine attends exclusively to the latter and expects the patient to keep the former out of the doctors’ way. But an increasing number of patients, lurking passively within observable bodies subject to external medical control, want to become active agents within experiential bodies subject to their own control.
The downfall of positivism
Medical science is one of the human sciences, and the limits of objectivist, quantitative research in the other human sciences have been well reviewed for many years. (Argyris, 1968. 1970; Bernstein, 1983; Gergen, 1973; Guba and Lincoln, 1994; Harré and Secord, 1972; Israel and Tajfel, 1972; Heather, 1976; Joynson, 1974; Lincoln and Guba, 1985; Reason and Rowan, 1981; Shotter, 1975; Smith, Harré, Van Langenhove, 1995; Braud and Anderson, 1998). I will give here a brief summary of some of the main criticisms.
The overarching criticism is that there is no external world, entirely independent of the researcher’s mind, against which to verify or falsify hypotheses:
The findings of the observer are shaped by the observer in interaction with the phenomena. This is evident both in the physical sciences and the social sciences.
So-called statements of objective fact are theory-laden. They can only be formulated within a pre-existing set of theoretical assumptions.
So-called statements of fact are also value-laden. The underlying theoretical assumptions which shape them represent values preferred to the values implicit in other rejected assumptions.
More specific criticisms relate to quantitative approaches that use inferential statistics, the control of selected variables through randomized designs, and imported categories of understanding. Their relevance to medical research is no less telling than it is in the other human sciences (Heron, 1986, 1996).
Selecting and controlling variables means the exclusion of others that are influential, and can involve discounting some of those that are selected and controlled. The resulting findings have little relevance to understanding how all the pertinent variables are at work in the real world.
This problem is chronic in medical research, which is designed to discount the influential variable of the placebo effect. The result is that modern medicine has no systematic grasp whatsoever of how the effect of mental attitude on bodily processes is at work in the real world of clinical practice, that is, in the day to day management of the therapeutic process.
Inferential statistics bury individual differences under comparisons of means, and throw no light on the idiosyncratic nature of individual responses.
In medical research, clinical trials assume the homogeneity of their research populations. The statistical method used hides what happens to individuals in the trial. With respect to two treatment groups, statistical analysis may show that one treatment is better than another, yet there may be some people in both groups who are worse after treatment. In general, medical research works to ‘obscure rather than illuminate interactive effects between treatments and personal characteristics’ (Weinstein, 1974). It can throw no light on the fact that individuals respond differently to the same treatment. Therefore it cannot help with the everyday clinical question ‘What is the treatment of choice for this individual patient?’
There is thus a mismatch between research method and clinical reality. The former assumes that patients are the same and obscures their differences, while the latter repeatedly reveals the patient differences that defeat this assumption. The inevitable result is a therapeutic culture which has a significant iatrogenic effect. Treatment based on conventional inferential statistics is bound sooner or later to harm some patients in ways that medical research can neither predict nor understand.
People cannot be understood either in terms of externally measured variables, or in terms of researcher imported categories. A full understanding of people necessarily includes the meanings and purposes they invest in their way of being and their actions, as these are interpreted through dialogue with them.
Medical research totally ignores the meanings and purposes which people invest in their experiential illnesses and attends exclusively to their observable diseases. By ignoring the intentionality of illness, the way people choose to feel it, construe it and do it, medical culture systematically and continuously disempowers people by regarding their subjectivity as irrelevant to their healing.
The methodology presupposes strict causal determinism. A model of relative indeterminism and autonomous agency is better suited to the explanation of human behaviour.
Medical culture treats people as patients contained within bodies subject to strict causal determinism, and as recipients of external therapeutic control. The placebo effect suggests, on the contrary, that people are autonomous agents who have within them the power to influence what goes on in their bodies, whose processes are therefore relatively indeterministic, or, which is the same thing, are only relatively determined by causal laws at the purely physical level.
A participatory worldview
The inquiry paradigm of objectivist Mechanos is breaking down because it cannot do justice, in an integrative way, to the full range of human experience in so many fields: medical research, the other academic human sciences, consciousness research, subatomic physics, systems research, ecology, and so on.
An emerging alternative inquiry paradigm is that of participative reality. This holds that there is a given cosmos in which the mind creatively participates, and which it can only know in terms of its constructs, whether experiential, imaginal, conceptual or practical. We know through this active participation of mind that we are in touch with what is other, but only as articulated by all our mental sensibilities. Reality is always subjective-objective: our own constructs clothe a felt participation in what is present. Worlds and people are what we meet, but the meeting is shaped by our own terms of reference. (Merleau-Ponty, 1962; Bateson, 1979; Reason and Rowan, 1981; Spretnak, 1991; Heron, 1992, 1996, 1998; Varela et al, 1993; Skolimowski, 1994; Reason, 1994a).
The participatory paradigm asserts that we cannot have any final or absolute experience of what there is: in the relation of knowing by face-to-face acquaintance, the experiential knower shapes perceptually what is there. And this is still so when the perceiving mind is relatively free of conceptual labels imposed upon its imaging of reality. However, the point about experiential knowing is that the very process of perceiving is also a meeting, a transaction, with what there is. To touch, see or hear something or someone does not tell us either about our self all on its own, nor about a being out there all on its own. It tells us about a being in a state of interrelation and co-presence with us.
When I hold your hand, my tactual imaging both subjectively shapes you and objectively meets you. To encounter being or a being is both to image it in my way and to know that it is there. Knowing a world is in this felt relation at the formative interface between a subject and what is met. To experience anything is to participate in it, and to participate is both to mould and to encounter. In the relation of meeting, my subjectivity becomes a perspectival window that frames and is filled with a world which also transcends it.
Hence experiential reality is always subjective-objective. It is subjective because it is only known through the form the mind, perceptually and conceptually, gives it; and it is objective because the mind interpenetrates the given cosmos which is shapes.There is an analogue here with Rahner’s modern theology of revelation, in which he speaks paradoxically of ‘mediated-immediacy’: we experience divine presence always in mediated form (Kelly, 1993).
Merleau-Ponty shows how perception itself is participatory so that
… in so far as my hand knows hardness and softeness, and my gaze knows the moon’s light, It is as a certain way of linking up the the phenomena and communicating with it. Hardness and softness, roughness and smoothness, moonlight and sunlight, present themselves in our recollection not pre-eminently as sensory contents but as certain kinds of symbioses, certain ways the outside has of invading us and certain ways we have of meeting the invasion. (Merleau-Ponty, 1964:317)
As Abram has it, this means that there is ‘underneath our literate abstractions, a deeply participatory relation to things and to the earth, a felt reciprocity….’ (Abram, 1996:124).
Or as Skolimowski puts it
Things become what our consciousness makes of them through the active participation of our mind (1994: 27-28).
The cosmos or the universe is a primordial ontological datum, while the ‘world’ is an epistemological construct, a form of our understanding. (1994: 100)
Bateson makes the point that between the extremes of solipsism, in which ‘I make it all up’, and a purely external reality, in which I cease to exist, there is
… a region where you are partly blown by the winds of reality and partly an artist creating a composite out of inner and outer events. (in Brockman, 1977: 245)
From all this it follows that what can be known about the given cosmos is that it is always known as a subjectively articulated world, whose objectivity is relative to how it is shaped by the knower. But this is not all: its objectivity is also relative to how it is intersubjectively shaped. For there is the important if obvious point that knowers can only be knowers when known by other knowers: knowing presupposes mutual participative awareness. It presupposes participation, through meeting and dialogue, in a culture of shared art and shared language, shared values, norms and beliefs. And, deeper still, agreement about the rules of language, about how to use it, presupposes a tacit mutual experiential knowing and understanding between people that is the primary ground of all explicit forms of knowing (Heron, 1996). So any subjective-objective reality articulated by any one person is done so within an intersubjective field, a context of shared meanings – at one level linguistic-cultural and, at a deeper level, experiential.
Critical subjectivity and four ways of knowing
A participative worldview, with its notion of reality as subjective-objective, involves an extended epistemology (Heron, 1992, 1996). A knower participates in the known, articulates and shapes a world, in at least four interdependent ways: experiential, presentational, propositional and practical. These four forms of knowing constitute the manifold of our subjectivity, within which, it seems, we have enormous latitude both in acknowledging its components and in utilizing them in association with, or dissociation from, each other. This epistemology presents us as knowers with an interesting developmental challenge, that of critical subjectivity. This involves an awareness of the four ways of knowing, of how they are currently interacting, and of ways of changing the relations between them so that they articulate a subjective-objective reality that is unclouded by a restrictive and ill-disciplined subjectivity.
Experiential knowing means direct encounter, face-to-face meeting: feeling and imaging the presence of some energy, entity, person, place, process or thing. It is knowing through participative, empathic resonance with a being, so that as knower I feel both attuned with it and distinct from it. It is also the creative shaping of a world through the transaction of imaging it, perceptually and in other ways. Experiential knowing thus articulates reality through felt resonance with the inner being of what is there, and through perceptually enacting (Varela et al, 1993) its forms of appearing.
Presentational knowing emerges from and is grounded on experiential knowing. It is evident in an intuitive grasp of the significance of our resonance with and imaging of our world, as this grasp is symbolized in graphic, plastic, musical, vocal and verbal art-forms. It clothes our experiential knowing of the world in the metaphors of aesthetic creation, in expressive spatiotemporal forms of imagery. These forms symbolize both our felt attunement with the world and the primary meaning embedded in our enactment of its appearing.
Propositional knowing is knowing in conceptual terms that something is the case; knowledge by description of some energy, entity, person, place, process or thing. It is expressed in statements and theories that come with the mastery of concepts and classes that language bestows. Propositions themselves are carried by presentational forms – the sounds or visual shapes of the spoken or written word – and are ultimately grounded in our experiential articulation of a world.
Practical knowing is knowing how to do something, demonstrated in a skill or competence. Practical knowledge is in an important sense primary (Heron, 1996). It presupposes a conceptual grasp of principles and standards of practice, presentational elegance, and experiential grounding in the situation within which the action occurs. It fulfils the three prior forms of knowing, brings them to fruition in purposive deeds, and consummates them with its autonomous celebration of excellent accomplishment.
It is equally important that action not only consummates the prior forms of knowing, but is also grounded in them. It is in this congruence of the four aspects of the extended epistemology that lie claims to validity. The bipolar relationship can be shown as in Figure 1.
Critical subjectivity means that we attend both to the grounding relations between the forms of knowing, and also to their consummating relations. It means that we do not suppress our primary subjective experience but accept that it is our experiential articulation of being in a world, and as such is the ground of all our knowing. At the same time, naively exercised, it is open to all the distortions of those defensive processes by which people collude to limit their understanding. So we attend to it with a critical consciousness, seeking to bring it into aware relation with the other three ways of knowing, so that they clarify and refine and elevate it at the same time as being more adequately grounded in it.
In addition, since our knowing is from a perspective and we are aware of that perspective, of its authentic value and of its restricting bias, we articulate this awareness in our communications. Critical subjectivity involves a self-reflexive attention to the ground on which one is standing. It also extends to critical intersubjectivity. Since our personal knowing is always set within a context of linguist-cultural and experiential shared meaning, having a critical consciousness about our knowing necessarily includes dialogue, feedback and exchange with others, and this leads to the methodology of co-operative inquiry.
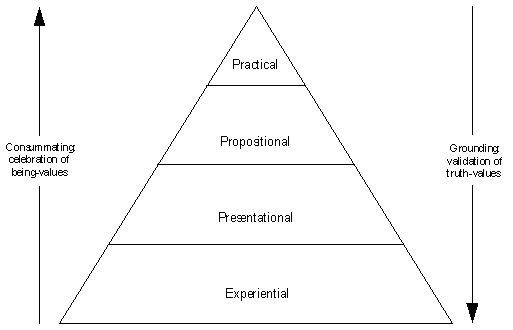
Figure 1: Bipolar congruence of four forms of knowing
Methodology: co-operative inquiry
The inquiry method within a participative worldview needs to be one which draws on this extended epistemology in such a way that critical subjectivity is enhanced by critical intersubjectivity. Hence a form of research in which all involved are both researchers and subjects: they engage together in democratic dialogue as co-researchers in designing, managing and drawing conclusions from the research, and as co-subjects they engage in the action and experience that the research is about (Heron,1971,1981a,1981b, 1985, 1988, 1992,1996; Heron and Reason, 1986, 2000; Reason, 1988a, 1994a, 1994b; Reason and Heron, 1995).
In such co-operative inquiry people collaborate to define the questions they wish to explore and the methodology for that exploration (propositional knowing); together or separately they apply this methodology in the world of their practice (practical knowing); which leads to new forms of encounter with their world (experiential knowing); and they find ways to represent this experience in significant patterns (presentational knowing) which feeds into a revised propositional understanding of the originating questions. Thus co-inquirers engage together in cycling several times through the four forms of knowing in order to enrich their congruence, that is, to refine the way they elevate and consummate each other, and to deepen the complementary way they are grounded in each other. In simple terms, people move, in successive cycles, from experience of a topic to shared reflection on it, which revises the way they next explore it experientially, and so on.
Research cycling is itself a fundamental discipline which leads toward critical subjectivity and a primary way of enhancing the validity of inquirers’ claims to articulate a subjective-objective reality. There are also a range of further of procedures which develop this effect. These include: managing divergence and convergence within and between cycles; balancing reflection and action; securing authentic collaboration; challenging uncritical subjectivity and intersubjectivity; managing unaware projections and displaced anxiety; attending to the dynamic interplay of chaos and order. These are mentioned in a little more detail later on. For a full discussion, together with a set of radical skills of being and doing required during the action phases of the inquiry, and for a comprehensive account of co-operative inquiry, see Heron (1996).
Co-operative inquiry has been applied in diverse fields: altered states of consciousness (Heron, 1998, 2000), black managers and subordinates, child protection supervision, co-counselling, co-operation between conventional and complementary practitioners (Reason, 1991), dental practitioners, district council organizational culture, health visitors, obese and post-obese women, other people with a particular physical or medical condition taking charge of how their condition is defined and treated, whole person medicine in general practice (Heron and Reason, 1985; Reason, 1988b), womens’ staff in a university, young women managers, youth workers, and more. For further references see Reason (1988a, 1994a), Heron (1996), Heron and Reason (2000).
Co-operative inquiry is related to other forms of participative inquiry such as action science (Argyris and Schon, 1974; Schon, 1983; Argyris et al, 1985), action inquiry (Torbert, 1991), participatory action research (Fals-Borda and Rahman, 1991), some forms of feminist inquiry (Mies, 1993; Olesen, 1994; Clements et al, 1998)), emancipatory action research (Carr and Kemmis, 1986), appreciative inquiry (Cooperrider and Srivastva, 1987), fourth generation evaluation (Guba and Lincoln, 1989), intervention research (Fryer and Feather, 1994), and others (Braud and Anderson, 1998; Bradbury and Reason, 2000). For how several of these differ from co-operative inquiry see Heron (1996).
The body as a subjective-objective reality
On the participatory worldview, a human body is not a purely objective reality, not something out there in the world quite independent of human subjectivity. It is a participatory reality, a subjective-objective reality, and the most basic sense in which this is so is in my knowing of my own body.
The experiential body
In terms of the fourfold epistemology outlined above, the grounding knowing of my body is in terms of experiential knowing, and the basis of this is proprioception: feeling from within the movement, posture and qualitative state of my body. This inner felt sense is spatiotemporal in form. It is the foundational knowing of my body as extended in space, moving – and pulsing rhythmically – in time. It is elaborated by how I image my body in all other sensory modalities, that is, by touching and seeing it and hearing it.
The subjective experience of my body is a proprioceptive imaging of it which is transactional. It ‘intermingles with’ and is, in some indeterminate measure, to some unknown degree, constitutive of my body. For the participatory worldview, my body is a reality which partially consists of my internal experience of it. Put another way, I co-create my body in and through my inner felt sense of, my spatiotemporal participation in, the cosmically given. The cosmos presents something which I shape up as the experience of indwelling a body in a world. I will call this inner felt sense of embodiment the experiential body. And the experiential body to some degree shapes the given body: this is the subjective-objective reality of the human body.
A polar, complementary way of knowing the given body is by external observation, elaborated by a whole range of physical instruments and interventions, and symbolized by verbal and numerical statements. This observable body – as known in natural science – is certainly not the given body in some external, absolute, objective sense. It is the given body as shaped by, and relative to, our observing and cognitive capacities in interaction with it. It is also a subjective-objective reality.
But the observable body can provide us with some grasp of how far the experiential body shapes the given body. We can use it, cautiously, as a mediate symbol, an external marker, of the interaction. We need to be cautious, simply because the observable body is in part constituted by the range of sensibilities and modes of cognition we deploy in framing it. Always remembering this, we can talk for convenience of how the experiential body does or does not shape the observable body.
Formative intentionality of the experiential body
The inner felt sense of my body is not merely passive receptivity. It is active-passive, intentional-responsive: with greater or lesser awareness I intend it. I shape my body by how I intend my spatiotemporal being in it, by how I move, gesture, posture, breathe, make sound, by how I qualitatively experience it, how I value and invest meaning in it, and by how I image it in other sensory modalities.
All these thing all the time are intentional, chosen, however relatively unaware the choice may be. It is this inherent and inalienable intentionality which is co-creative with cosmic creativity. We may have made some adaptive survival choices early in our life, which become so habitual we lose any sense of them being choices and kid ourselves they are just our given body. But that they are choices becomes clear when we realize that we can unchoose them and become awarely purposive about changing the way we are doing, being in, shaping our bodies.
Furthermore, every subtle micro-choice about how we do our embodiment, is a preference for one way of doing it over another. Each such preference is an embodiment of one emotional value favoured over another that is discarded. Emotional appraisal is the very stuff of rapid decision-making (Goleman, 1996). On this account, emotional attitude is formative of the experiential body, and so to some degree the observable body. Hence the significance of the new area of psychoneuroimmunology (Cousins, 1990).
On the participatory worldview, all these things – how I move, gesture, posture, breathe, make sound, how I qualitatively experience my body, emotionally value and invest meaning in it, image it in other sensory modalities – shape what we come to know analytically and propositionally in more external terms about body. What we do not yet in any great detail know is how much they do and can shape what we know about the externally observable body. We do not know how much the cosmos insists on its own ontological datum, its own agenda of creation.
Formative intentionality of illness and of recreating wellness
It follows from all the above, that any observable disease, from the standpoint of the participatory paradigm, is in part shaped by its correlative subjective experiential illness: how the person is spatiotemporally doing and being in, investing emotional value and meaning in, imaging in all sensory modalities, his or her ill experiential body. What the still prevalent Cartesian paradigm does is to create a cultural climate in which people continually discount the way in which the unacknowledged intentionality of their illness is to some degree shaping their externally observable disease. The patient occludes this inner intentionality by relying on the external authority of the doctor, and thus relinquishes any sense of himself or herself as an agent whose illness is affecting the disease, and who potentially has an unexercised, unexplored and unknown capacity to change this process.
If all subjective illness is implicitly intentional and as such in part shapes observable disease, then raising consciousness about this and being explicitly intentional with full awareness about how I am spatiotemporally doing, emotionally valuing and meaning, my embodiment, has the potential to reshape observable disease. The first step is to raise my awareness of and identify my past and current way of doing all this. The second step is to change these ways in a significant manner: I recreate how I move, gesture, posture, breathe, make sound, how I qualitatively experience my body, emotionally value and invest meaning in it, image it in other sensory modalities. This now extends to how I heartbeat, rest-exert, sleep-wake, ingest-excrete, how I do all the other micro and macro rhythms of embodiment. I set out to change the experiential illness into experiential wellness and expect thereby to modify observable disease processes.
This is intentional self-healing. Its potential capacity is at present unknown. The current labelling of certain observable diseases as incurable rests on the unstated, conspiratorial Cartesian assumption that their concomitant experiential illnesses have no relevance either to their aetiology or their treatment. The question-begging stated assumption is that these diseases will remain incurable until a purely physical remedy or procedure is found.
Because the degree to which the unacknowledged intentionality of illness shapes externally observable disease is unknown, the implications of the participatory paradigm need to be used with consideration and caution. We are not entitled to make the diseased feel inadequate and guilty by telling them dogmatically that their diseases are nothing but the effects of their unowned states of mind. It is an oppressive question-begging assumption that a given disease in its entirety is a product of tacit intentional experiential illness and is fully reversible. The most we are entitled to do is put forward the hypothesis that it may to some degree be such a product, and to invite those for whom this idea seems plausible and relevant to their own condition to explore it in active practice.
Symbolizing the experiential body
Everything which anyone comes to know about the observable body in terms of propositional knowledge – anatomy, biochemistry, physiology, aetiology and pathology – rests on and presupposes the subjective experience of indwelling a body. Each observer’s external account rests on a prior experiential knowing of the body of the observer, a subjective knowing which necessarily forever falls outside, and is always presupposed by, the terms and methods of the external observation. In short, my experiential body is the ground of and is irreducible to my knowledge of the observable body. Put in another way, the observable body is a marker of how it is to some degree shaped by the experiential body, never an explanation of the presence or power of the experiential body.
My felt experience of indwelling a body cannot be described in statements based on external, analytic observation; that is, in terms of kinaesthetic relays from neural sites in the joints, muscles and so on. Such statements neither describe it nor explain it, they only provide details of its bio-mechanical concomitants. The experiential body is first and foremost symbolized in its own terms, and most accessibly, through my movement, posture, gesture and mode of breathing. How I am embodying myself I directly convey in these presentational forms, which have their own inherent emotional meaning.
To raise my consciousness about the sort of tacit intentionality at work in my experiential body I need to have presentational knowledge of myself, that is, I need to notice how my movement, posture and gesture and mode of breathing symbolize how I am choosing to embody myself. I need to notice what these living symbols tell me about the emotional value and meaning I invest in my being in a body. This can then develop into the creative intentionality of the experiential body: a conscious artistry of personal motion, through which a person chooses awarely to symbolize the emotional meaning and value they give to embodied life by how they move, gesture, posture, make sound, breathe, and intend all the other micro and macro rhythms of the experiential body. The foundation of intentional wellness and self-healing, on this view, is to do with the radical connection between life, motion, spatiotemporal form and rhythm, intentionality and emotional attitude.
The formative power of others’ experiential knowing
You participate in the subjective-objective reality of my body by experientially knowing it: by perceptually imaging it and intuiting the meaning of its movements, sounds, postures and gestures, and through empathic resonance with my experience of indwelling it.
This participative knowing of my body is also subjective-objective transaction, which means that it too is to some unknown degree formative. Perceiving another person and empathically resonating with their experience influences and shapes the subjective-objective reality of their body. This effect may (or may not) be minimal compared to the intentionality of that person in co-creation with the shaping power of the cosmically given, but, for the participatory paradigm it is there.
This means that the experiential encounter between medical practitioner and patient can have some effect both on the patient’s illness and on their observable disease. Furthermore, a practitioner, when experientially present to a patient, can resonate and attune not only to how the person is actually being in their body, but also with their as yet unexplored potential for being in it in creative, transforming ways. Hence the power of satsang, of being with the healer whose attuned presence elicits self-transformative energy in the patient.
The primary impact of the practioner-patient relationship, on this view, lies in the way the practitioner perceptually images, resonates and is present with the patient, rather than on what is said. But what is said by the practitioner will have a powerful secondary impact, when it is rooted in and emerges from the primary impact of such presence.
Supportive data
There is a lot of data lying around in support of the participatory view of the body as a subjective-objective reality, whose intentional subjectivity is in part constitutive of it and has power to some unknown degree to influence its processes. There is, of course, the placebo effect: the fact that believing an ingested substance will have a bodily effect makes it have that effect. There is the impact of human intention on bodily processes mediated externally by biofeedback devices; and mediated internally by autogenic training, relaxation, visualization and meditation, control of movement and breathing. There is the powerful influence of posthypnotic suggestion on the reversal of functional and structural bodily disorder. And there are cases of attitudinal healing in which an intentional transformation of an internal attitude of mind leads to a reduction or elimination of obervable disease process.
There is also growing support for the participatory view of the influence on outcomes of the experiential encounter between practitioner and patient. Medical education and primary care practice underline the importance and value of the doctor-patient relationship, and studies show significant patient differences in response to how it is handled (Cousins, 1990). Psychotherapy research indicates it is the therapists’ qualities of personal presence brought to the therapeutic interaction which have a greater effect on outcomes than any therapeutic techniques. Some complementary therapists seek a charismatic engagement with their patients and claim this empowers radical life-style changes in them.
The relevance and limits of conventional medical research
All this data, both experimental and anecdotal, is sufficiently well documented and creditable, in terms of the participatory paradigm, to call for further research. The question is: what sort of research? Conventional medical research methods can be, and have been, with good effect, used to compare a group of people who have some disease and who practice intentional self-help with matched controls who are having no treatment and/or some conventional treatment (Cousins, 1990).
The design needs to be non-randomized, with matched controls selected from the records of centres of excellence. The use of a controlled trial with random allocation entails a moral obligation to seek the informed consent of people to participate in the trial. This means asking people to agree to the possibility of being randomly allocated to a control group in which they are not to practise intentional self-healing. Apart from the dubious morality of this request, it is self-defeating, since the very making of it is a powerful suggestion which undermines it. So medical research using randomized designs is faced with a strong dilemma. If it tries to explore patient intentionality it disempowers itself; if it maintains its own authority, it ignores and disempowers patient intentionality.
A non-randomized approach yields useful external data comparing observable disease processes in the intentional self-healing group and a no treatment or conventional treatment group. But the use of conventional research design and statistical analysis can not tell us anything at all about:
The internal strategies, the subjective processes, of intentional self-healing as such: that is, the practical knowledge involved in know how to do it
Individual differences among patients with respect to effective strategies.
The therapeutic effect understood as a dynamic pattern of the main influential variables: patient intentionality, psychosocial context, observable disease process, co-patient interaction, relationships with health care professionals, and external remedies and procedures used. (Heron, 1996).
The relevance of co-operative inquiry
All these things can only be addressed if we cease to think of ill people as patients and regard them as intentional agents and invite them to become active in the inquiry process.
Agents, hitherto called patients, become members of a co-operative inquiry, along with relevant health care professionals and co-operative inquiry initiators. They become co-inquirers as well as co-subjects since their agency and their mental states are key variables which can only properly be used, and the use of which can only be properly understood, if as agents they participate in deciding how and why they are to be used.
Self-healing, as intentional process, can only be researched by those who are busy with their own subjectivity and at the same time busy with critical subjectivity, as defined earlier. Internal agency, as practical knowing how, can only be investigated by the agents concerned. And they need to collaborate in their inquiry with each other, for critical subjectivity means also, as we have seen, critical intersubjectivity.
Agents are involved not only in acquiring practical knowledge of self-help methods. They also, along with relevant health care professionals in the inquiry group, seek to understand the role of self-help in the total pattern of influential variables, such as those listed above, and to grasp what whole pattern makes for a significant effect on both experiential illness and observable disease. The co-inquirers come to this understanding through cycles of action and reflection, varying the pattern in the action phases, and on the basis of this experience learning, in the reflection phases, to discriminate what makes for a healing pattern. The validity of the pattern is inherent in its organization, which can only be studied from within it (Reason, 1986). Thus the influential variables are not split between an experimental and a control group, but all of them are studied together in the inquiry group.
Agents are involved in understanding the participatory worldview as a shared worldspace, an intersubjective way of experiencing and construing reality. The more the participatory worldview is made explicit, the more people together co-operate in empowering their subjectivity by putting the paradigm to work, the more potent that subjectivity is likely to become.
The outcome of all this is a form of participative medical research in which illness is seen as a way in which people articulate their reality, and as a project which can be restructured to influence their observable disease, or to transform their experiential illness, or both.
A co-operative inquiry project
As mentioned above, co-operative inquiry has so far been used in the health arena in two ways: among healthcare professionals, of the same or different kinds, looking together at their work; and among peer groups of people with a particular physical or medical condition taking charge of how their condition is defined and treated. To my knowledge there has been no small or large scale use of full-blown co-operative inquiry with a group of patients who have been invited to revision themselves as potential self-healing agents and who are co-inquirers with their relevant healthcare professionals. For an early proposal about a related project, see Reason and Heron (1986).
Obstacles
One obvious reason why the challenge has not been met, is that the inquiry methodology is not well known, its underlying paradigm is not understood, and its social and political implications are a potential threat. Medical researchers still uncritically wedded to, and restricted by, the positivist paradigm strongly resist the idea that there can be any alternative method. This is buttressed by the fact that all forms of participatory research which include patients as self-directed co-researchers, threaten the political hegemony of conventional medicine in controlling patients’ lives.
However some radical practitioners intuitively shift in the direction of participative research. Schneider’s work with clients is on the edge of informal co-operative inquiry, as is his vision for the future of a self-healing community (Schneider, 1987). All healing centres in which practitioners and their clients adopt a non-dogmatic, co-operative approach to the healing process are also incipient, inchoate co-operative inquiries. This applies, too, to peer self-help groups of patients with similar complaints.
Another obstacle, of course, is the demoralizing climate created in contemporary society by the powerfully publicized prevalence of the Cartesian medical model. Patient subjectivity is downgraded and regarded as an embarrassing irrelevance, for both patient and doctor, to the purely technical project of physical medicine. In terms of the participatory paradigm, such a pervasive intersubjective belief system will have an influential negative, depressing effect on patient subjectivity and its potential for self-healing.
The effect may indeed go further. The Cartesian model, by putting it about that some diseases are autonomous faults waiting around, independent of our minds, incurably to overcome some of our bodies, may cause some people, through fear, mentally to induce them. It is not simply that the practical application of modern medicine has inescapable iatrogenic effects. Its underlying paradigm, per se, may also have such effects: it may not only paralyze self-healing, it may induce experiential illness and hence observable disease. All this follows from the participatory worldview that we both subjectively and intersubjectively articulate and shape our realities.
A third and related obstacle is well-known human resistance to self-development: those who find it convenient not to notice and own the negative attitudes that shape their way of being embodied, will have the usual kinds of denial to dismantle before launching intentional transformation.
Membership and roles
For these sorts of reasons, patients wanting to join a co-operative inquiry about intentional self-healing need to self-select themselves carefully: they are not too debilitated, are willing to take up the participatory paradigm and rebuff the Cartesian medical model, open to inquiry, not deluded by unwarranted assumptions, not too resistant, willing to develop their own practical knowing how to be embodied.
A co-operative inquiry project about intentional self-healing would involve self-selected patients, relevant healthcare professionals, and co-operative inquiry initiators. Everyone in the project would be involved in the thinking and planning that designs the inquiry, manages its ongoing process, and draws conclusions from it. Everyone would also be involved in the action and experience being researched, that is, in the chosen intentional practices, either to transform experiential illness in patient members or to enhance experiential wellness in nonpatient members. The nonpatient members cannot properly understand and grasp the nature of, and make decisions about, intentional practices, and their dynamic relation to other factors, unless they engage in them themselves.
The project might go through the following stages. The very detailed account which follows is purely conjectural. In reality, the inquiry would be co-operatively designed and managed, step by step.
First reflection meeting
This first reflection meeting might indeed extend over several meetings. The co-operative inquiry initiators would facilitate and guide these early meetings, and support the group in evolving basic concepts in basic English. They may offer tentative conceptual frameworks as a basis for consultation within the group.
The group develops a provisional working model of how human intention and subjectivity mould bodily process and form; of the tacit intentionality of experiential illness and its relation to observable disease; of bedrock intentional ways of transforming experiential illness into experiential wellness, and of enhancing experiential wellness.
The group agree a provisional working model of all the main influential variables as well as intentional agency, and a provisional model of an effective life-enhancing pattern of interaction among them. Such variables may include: intentional agency (self-help techniques), psychosocial context, observable bodily process, co-agent interaction (between patients, between nonpatients, between patients and nonpatients) and external remedies and procedures used.
The group agree criteria for defining and recording the state of the subjective, experiential body of all those involved in the project. This includes the experiential illness of the patients, and the relative experiential wellness of the nonpatient members. This recording is done.
The group agree criteria for defining and recording the state of the external, observable body with regard to the observable disease of the patient members, and along the same paramaters, the observable bodily integrity of the nonpatient members. This recording is done.
The group agree on the range of self-directed techniques for recovery from illness and for enhancing wellness, and practice together the skills involved. They also agree on ways of monitoring and recording the ongoing use of these techniques and their apparent effects, both subjective and observable. Individual inquirers then choose the particular techniques each is motivated to use for the first phase of application.
The group agree on their time framework: how long each phase of application will be, and how long each intervening meeting for review, reflection and further planning will be; and how many cycles of application and reflection there will be overall.
Cycles of inquiry
The group now embark on the agreed series of inquiry cycles.
In the first application phases, everyone is busy applying their chosen self-directed techniques of intentional self-healing and enhanced wellbeing, in the context of the agreed pattern of other influential factors. They are also keeping records, as agreed above, of the use and apparent effects of these and their contextual pattern.
At the next reflection meeting, all this data is shared and made sense of within the whole group. In the light of this, group members revise the several decisions made at the first reflection meeting, and plan the next application phase to take account of these revisions.
In similar manner, the co-inquirers proceed through the remaining inquiry cycles, moving from appplication phases to reflection and forward planning meetings. Progressively, cycle by cycle, group members modify and extend the use of self-directed techniques, accumulate data about their effects, refine and amend the model of how all the relevant influential factors may fruitfully interact.
During these cycles, the co-operative inquiry initiators will prompt the group to take time out to review validity issues, for a full discussion of which see Heron (1996). They include:
Managing divergence and convergence within and between cycles. This attends to whether people are doing the same or different things within a given application phase; also in this application phase compared to the previous one. The balance between divergence and convergence relates to the balance between partitive and holistic accounts of the inquiry topic.
Balancing reflection and action. This means checking that there is neither too much time spent on application in relation to time spent on reflection, nor vice versa.
Securing authentic collaboration. This is done by attending regularly to the right of each participant to have a genuine say in all aspects of research decision-making, and to engage fully in the application phases of the inquiry.
Challenging uncritical subjectivity and intersubjectivity. One basic method is the adoption of some form of devil’s advocate procedure in which time is taken by any group member to confront possible collusion, delusion and illusion.
Managing unaware projections and displaced anxiety. This means attending to and clearing emotional and interpersonal distress activated by the inquiry process.
Attending to the dynamic interplay of chaos and order. This involves tolerating phases of uncertainty, disorder and confusion, allowing authentic order to emerge in its own good time out of chaos, without rushing anxiously into premature closure.
Completing the inquiry
The concluding reflection meeting, or series of meetings, will draw together the threads of the inquiry.
The co-inquirers, patient and nonpatient, record their end states of experiential illness and experiential wellness, and of observable disease and observable bodily integrity; and compare these with the opening – and any intermediate – records.
They exercise, on the basis of the accumulated experiential data, a final discriminating judgment about the pattern of influential factors that has been effective in any way. This will include, in particular and of special interest, the weight to be given to the use of intentional self-help techniques, as well as the other factors. Both common and idiosyncratic findings are honoured, for both patient and nonpatient members.
It is important to grasp here that what constitutes a valid effect – the interacting pattern of all the relevant influential variables – cannot be understood by selecting and controlling them and splitting them up between different groups, as in conventional positivist research. Nor can they be understood by someone, who is not involved in their use, but is seeking to control their total interaction without selection and splitting. Since they centrally include intentional subjectivity, they can only be understood by those who are busy with it, that is, by co-researchers who are also co-subjects. Getting hold of this idea is one of the main stumbling blocks for positivist researchers.
It is also interesting to note that similarities and differences – of techniques used, their effects, their relation to other influential factors – between patient and nonpatient members of the inquiry, will be hepful in clarifying, for both groups, an understanding of all these things.
They refine their practical knowledge of effective intentional self-healing techniques, and prepare some descriptive guidelines for their use.
In the light of all the above, they refine their original working model of how human intention and subjectivity mould bodily process and form; of the tacit intentionality of experiential illness and its relation to observable disease; of intentional ways of transforming experiential illness into experiential wellness, and of enhancing experiential wellness.
They review the validity of their findings in the light of their use of validity procedures and their skills in exercising critical subjectivity and critical intersubjectivity.
They plan how to prepare some co-operative report on the whole project. All co-inquirers read, edit and offer amendments to any initial draft; and all agree the final version.
While a written report is valuable and useful, the primary outcome of the inquiry is the range of practical knowledge gained by the co-inquirers: that is, the skills involved in using intentional self-healing and self-development; and the skills involved in harnessing them within a total pattern of effective life-enhancing endeavour. Furthermore, from the viewpoint of the participatory paradigm, of a subjective-objective reality, any written findings have only contextual validity, that is their validity is relative to the inquiry group that generates them and to its articulation of reality. They are not generalizable in the traditional positivist sense of external validity. They are only suggestive guidelines for other similar groups with similar interests to devise their own action-oriented inquiry and articulate their own reality.
8540 words, excluding introductory outline and references.
Abram, D. (1996) The Spell of the Sensuous. New York: Pantheon.
Argyris, C. (1968) ‘Some unintended consequences of rigorous research’, Psychological Bulletin, 70: 185-97.
Argyris, C. (1970) Intervention Theory and Method: A Behavioural Science View. Reading, MA: Addison Wesley.
Argyris, C. and Schön, D. (1974) Theory in Practice: Increasing Professional Effectiveness. San Francisco: Jossey-Bass.
Argyris, C. Putnam, R. and Smith, M.C. (1985) Action Science: Concepts, Methods nd Skills for Research and Intervention. San Francisco: Jossey-Bass.
Bateson, G. (1979) Mind and Nature: A Necessary Unity. New York: Dutton.
Bernstein, R.J. (1983) Beyond Objectivism and Relativism. Oxford: Basil Blackwell.
Bradbury, H. and Reason, P. (eds) (2000) Handbook of Action Rsearch. Thousand Oaks, CA; Sage.
Braud, W. & Anderson, R. (eds) (1998) Transpersonal Research Methods for the Social Sciences: Honoring Human Experience. Thousand Oaks, CA: Sage.
Brockman, J. (ed) (1977) About Bateson. New York: Dutton.
Carr, W. and Kemmis, S. (1986) Becoming Critical: Education, Knowledge and Action Research, Basingstoke: Falmer Press.
Clements, J., Ettling, D., Jenett, D. & Shields, L. (1998) ‘Organic research: feminine spirituality meets transpersonal research’, in W. Braud & R. Anderson (eds) Transpersonal Research Methods for the Social Sciences: Honoring Human Experience. Thousand Oaks, CA: Sage.
Cooperrider, D. L. and Srivastva, S. (1987) ‘Appreciative inquiry in organizational life’, in R. Woodman and W. Pasmore (eds) Research in Organizational Change and Development, Vol 1. Greenwich: JAI Press.
Cousins, N. (1990) Head First: The Biology of Hope and the Healing Power of the Human Spirit. New York: Penguin.
de Cuevas, J. (1995) ‘The Pleasing Placebo’, article on the internet, copyright President and Fellows of Harvard College.
Fals-Borda, O. and Rahman, M.A. (eds) (1991) Action and Knowledge: Breaking the Monopoly with Participatory Action Research. New York: Intermediate Technology/Apex.
Fryer, D. and Feather, N.T. (1994) ‘Intervention Techniques’, Qualitative Methods in Organizational Research. London: Sage.
Gergen, K.J. (1973) ‘Social psychology as history’, Journal of Personality and Social Psychology, 26: 309-20.
Goleman, D. (1996) Emotional Intelligence. London: Bloomsbury.
Guba, E.G. and Lincoln, Y.S. (1989) Fourth Generation Evaluation. Newbury Park, CA: Sage.
Guba, E.G. and Lincoln, Y.S. (1994) ‘Competing paradigms in qualitative research’, in N.K. Denzin and Y.S. Lincoln (eds) Handbook of Qualitative Research. Thousand Oaks, CA: Sage.
Harré, R. and Secord, P.F. (1972) The Explanation of Social Behaviour. Oxford: Basil Blackwell.
Heather, N. (1976) Radical Perspectives in Psychology. London: Methuen.
Heron, J. (1971) Experience and Method. Guildford: University of Surrey.
Heron, J. (1981a) ‘Philosophical basis for a new paradigm’, in P. Reason and J. Rowan (eds) Human Inquiry: A Sourcebook of New Paradigm Research. Chichester: Wiley.
Heron, J. (1981b) ‘Experiential research methodology’, in P. Reason and J. Rowan (eds) Human Inquiry: A Sourcebook of New Paradigm Research. Chichester: Wiley.
Heron, J. (1985) ‘The role of reflection in co-operative inquiry’, in D. Boud, R. Keogh and D. Walker (eds) Reflection: Turning Experience into Learning. London: Kogan Page.
Heron, J. (1986) ‘Critique of conventional research methodology’, Complementary Medical Research, 1(1): 12-22.
Heron, J. (1988) ‘Validity in co-operative inquiry’, in P. Reason (ed) Human Inquiry in Action. London: Sage.
Heron, J. (1992) Feeling and Personhood: Psychology inAnother Key. London: Sage.
Heron, J. (1996) Co-operative Inquiry: Research into the Human Condition. London: Sage.
Heron, J. (1998) Sacred Science: Person-centred Inquiry into the Spiritual and the Subtle. Ross-on-Wye: PCCS Books.
Heron, J. (2000) ‘Transpersonal co-operative inquiry’, in H. Bradbury and P. Reason (eds) Handbook of Action Rsearch. Thousand Oaks, CA; Sage.
Heron, J. and Reason, P. (1985) Whole Person Medicine: A Co-operative Inquiry. London: British Postgraduate Medical Federation.
Heron, J. and Reason, P. (1986) ‘Research with people’, Person-centered Review, 4(1): 456-76.
Heron, J. and Reason, P. (1997) ‘A participatory inquiry paradigm’, Qualitative Inquiry, 3(3): 274-294.
Heron, J. and Reason, P. (2000) ‘Co-operative inquiry’, in H. Bradbury and P. Reason (eds) Handbook of Action Rsearch. Thousand Oaks, CA; Sage.
Heron, J. and Reason, P. (1997) ‘A participatory inquiry paradigm’, Qualitative Inquiry, 3(3): 274-294.
Israel, J. and Tajfel, H. (eds) (1972) The Context of Social Psychology: A Critical Assessment. New York: Academic Press.
Joynson, R.B. (1974) Psychology and Common Sense. London: Routledge and Kegan Paul.
Kelly, G.B. (1993)Karl Rahner: Theologian of the Graced Search for Meaning. Edinburgh: Clark.
Lincoln, Y.S. and Guba, E.G. (1985) Naturalistic Inquiry. Beverly Hills, CA: Sage.
Merleau-Ponty, M. (1962) Phenomenology of Perception. London: Routledge and Kegan Paul.
Olesen, V. (1994) ‘Feminisms and models of qualitative research’, in N.K. Denzin and Y.S. Lincoln (eds) Handbook of Qualitative Research. Thousand Oaks, CA: Sage.
Reason, P. (1986) ‘Innovative research techniques’, Complementary Medical Research, 1(1): 23-39.
Reason, P. (1988a) (ed.) Human Inquiry in Action. London: Sage.
Reason, P. (1988b) ‘Whole person medical practice’, in P. Reason (ed.) Human Inquiry in Action. London: Sage.
Reason, P. (1991) ‘Power and conflict in multi-disciplinary collaboration’, Complementary Medical Research, 5(3): 144-50.
Reason, P. (1994a) (ed.) Participation in Human Inquiry. London: Sage.
Reason, P. (1994b) ‘Three approaches to participative inquiry’, in N.K. Denzin and Y.S. Lincoln (eds) Handbook of Qualitative Research. Thousand Oaks, CA: Sage.
Reason, P. and Heron, J. (1986) ‘The human capacity for intentional self-healing and enhanced wellness: a research proposal’, The British Journal of Holistic Medicine, 1(2): 123-34.
Reason, P. and Heron, J. (1995) ‘Co-operative inquiry’, in J.A.Smith, R. Harré and L. Van Langenhove (eds) Rethinking Methods in Psychology. London: Sage.
Reason, P. and Rowan, J. (1981) (eds) Human Inquiry: A Sourcebook of New Paradigm Research. Chichester: Wiley.
Schön, D. (1983) The Reflective Practitioner: How Professionals Think in Action. New York: Basic Books.
Shotter, J. (1975) Images of Man in Psychological Research. London: Methuen.
Skolimowski, H. (1994) The Participatory Mind. London: Arkana.
Smith, J.A., Harré, R., and Van Langenhove, L. (eds) (1995) Rethinking Psychology. London: Sage.
Spretnak, C. (1991) States of Grace: The Recovery of Meaning in the Postmodern Age. New York: Harper Collins.
Torbert, W.R. (1991) The Power of Balance: Transforming Self, Society and Scientific Inquiry. Newbury Park, CA: Sage.
Varela, F., Thompson, E., and Rosch, E. (1993) The Embodied Mind. Cambridge, MA: MIT Press.
Weinstein, J. (1974) ‘Allocation of subjects in medical experiments’, New England Journal of Medicine, 291: 1278-85.